

How to Treat Perioral Dermatitis and What Makes It Worse
Last updated on April 18th, 2026 at 03:43 pm
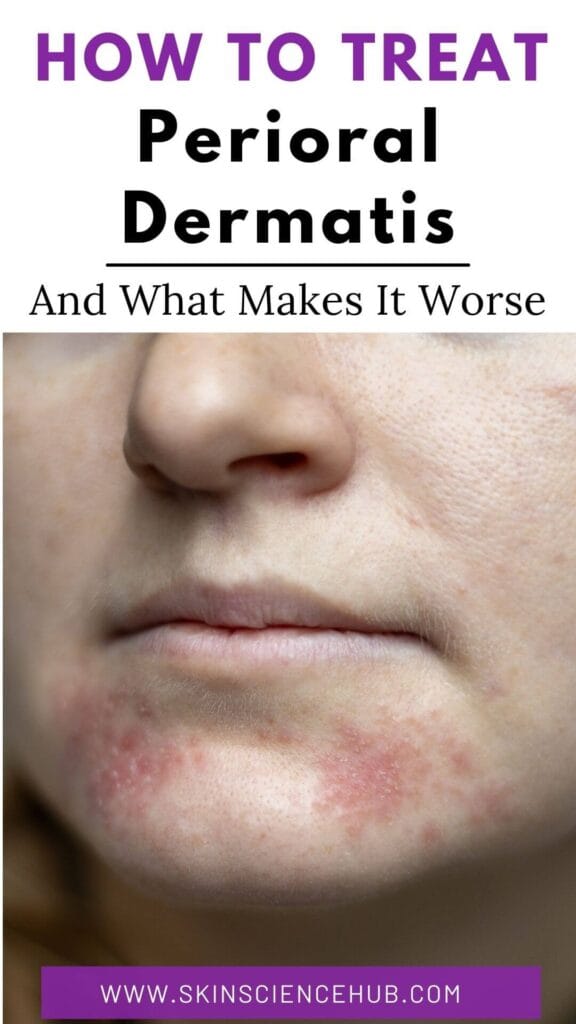
Red bumps cluster around your mouth, and acne treatments aren’t working. You may have perioral dermatitis.
This condition mimics acne and rosacea closely enough that most people spend months treating the wrong thing. Steroids clear the rash for a few days, then cause brutal rebounds when you stop. Heavy creams feel soothing but feed the inflammation. The products that seem logical are often the exact triggers keeping the rash alive.
As a pharmacologist, I understand what drives this condition, and once you know the mechanism, the treatment makes sense.
Perioral Dermatitis Symptoms and What to Look For
Perioral dermatitis causes small red bumps clustered around your mouth, nose, or eyes. The bumps group together rather than spreading evenly, and you might see pustules alongside them or just bumps with scaling and dryness.
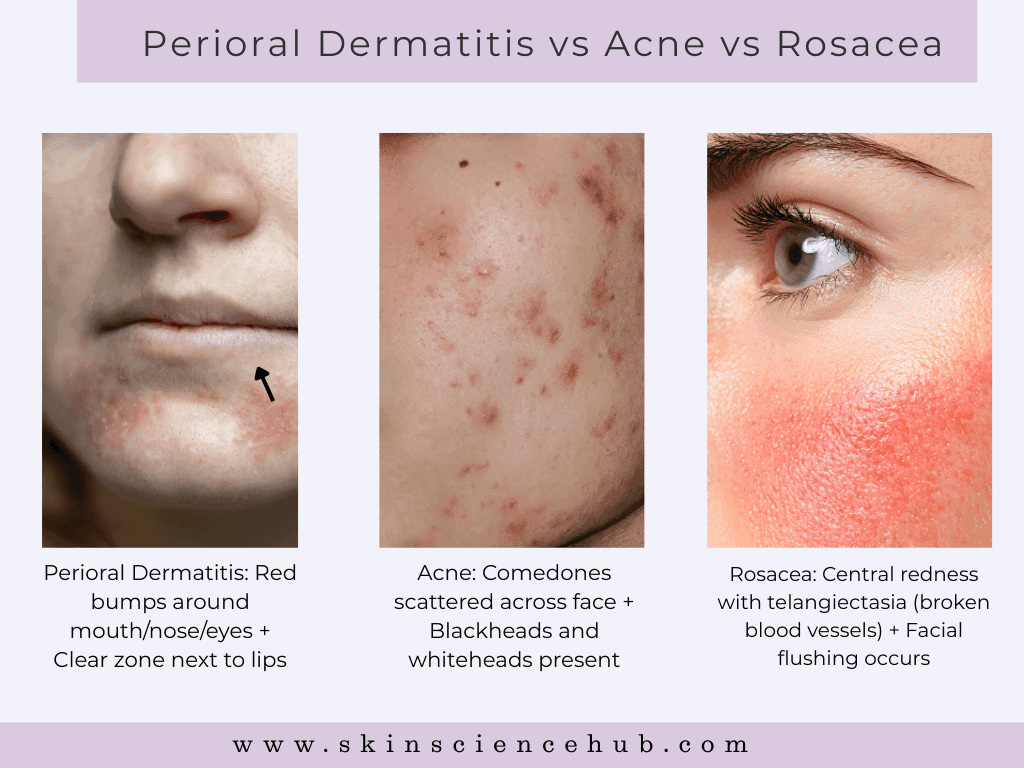
Bumps circle your lips yet spare the skin directly beside your mouth, creating a clear zone that separates perioral dermatitis from acne and rosacea. They may also appear around your nostrils or eyes, but rarely on your forehead or cheeks. When bumps appear around multiple areas, doctors call this periorificial dermatitis, though it’s the same condition with the same treatment.
Some people feel burning or stinging, while others notice no discomfort at all. Many cases cause zero symptoms beyond the visible bumps.
Not acne. You won’t see blackheads or whiteheads with perioral dermatitis. Acne also spreads across your face, chest, and back, whereas perioral dermatitis clusters around specific areas. If you have comedones, this isn’t perioral dermatitis.
Not rosacea. Rosacea causes flushing and visible broken blood vessels across your central face including your forehead. Perioral dermatitis spares your forehead entirely and creates that distinctive clear zone around your lips.
If you’ve been treating suspected acne or rosacea without success, perioral dermatitis may be what you’re dealing with. The treatments are completely different, and getting the right diagnosis is where clearing it starts.
A note on skin tone. Fair skin shows classic red papules and pustules. Darker skin shows the same bumps, but they appear brown or hyperpigmented. Melanin masks the redness, and this can delay diagnosis if your dermatologist has limited experience with skin of color. Look for the distribution pattern, not just the color.
Is Perioral Dermatitis Fungal or Bacterial?
Neither, and understanding this is what makes treatment make sense.
Perioral dermatitis is not a fungal infection, so antifungal creams won’t clear it. It’s also not a straightforward bacterial infection, so standard acne antibiotics applied topically don’t reliably work either. What it involves is a damaged skin barrier that creates the conditions for bacterial imbalance.
Your skin barrier is a layered structure of lipids and proteins that keeps irritants out and moisture in. When something disrupts it, whether a topical steroid, a heavy moisturizer, or fluoride residue sitting on your skin, the barrier breaks down. Moisture escapes, inflammatory substances penetrate deeper, and bacterial populations in your pores shift. Bacteria that normally live harmlessly on your skin multiply when this happens, and that overgrowth drives the redness and bumps you see.
This is why perioral dermatitis responds to certain antibiotics at low doses, not because they kill bacteria outright, but because they reduce inflammation and calm the immune response driving the bumps. And it’s why removing the trigger comes first. The barrier can repair itself once you stop what’s damaging it.
What Causes Perioral Dermatitis and Why It Starts Suddenly
The exact cause of perioral dermatitis remains unknown, but the triggers are well established. Topical steroids rank as the strongest, followed by fluoride toothpaste, heavy moisturizers, and cosmetics.
1. Topical Steroids
Topical corticosteroids show the strongest association with perioral dermatitis. The pattern is consistent. You apply hydrocortisone for mild irritation, it works for a few days, you stop, and the rash returns. Each cycle makes the condition more stubborn.
Steroids suppress inflammation but systematically dismantle your barrier in the process, reducing barrier lipids, thinning your outer skin layer, and shifting the bacterial populations in your pores. Each application weakens the barrier further, so when you stop, the rash rebounds harder than before.
Inhaled steroids for asthma and nasal steroid sprays also trigger perioral dermatitis, not just creams applied directly to your face.
Stopping steroids safely – Quitting abruptly triggers severe rebound flares. Reduce application from daily to three times weekly, then twice weekly, then once weekly before stopping completely. Some dermatologists prescribe pimecrolimus cream during the transition to manage rebound inflammation. You need to stop completely for perioral dermatitis to clear.
2. Fluoride Toothpaste
Fluoride consistently triggers perioral dermatitis, though the exact mechanism isn’t fully understood. Brushing twice a day means constant exposure, and residue sitting around your mouth maintains ongoing irritation.
Sensodyne, Pronamel, and prescription strength toothpastes all contain fluoride. Most mouthwashes do too. Switch to a fluoride-free alternative and wash around your mouth after brushing to remove any residue.
3. Moisturizers and Cosmetics
Heavy moisturizers create occlusive seals that prevent normal barrier function. Petrolatum, mineral oil, and isopropyl myristate are the main offenders. Bacteria multiply in the trapped environment underneath, and that overgrowth feeds the inflammation.
Research shows foundation combined with moisturizer creates thirteen times the risk compared to moisturizer alone. Layering occlusive products prevents your compromised barrier from recovering.
Sunscreens also trigger flares. Oil-based formulas and chemical UV filters like avobenzone and oxybenzone penetrate compromised barriers and cause irritation. Mineral sunscreens with zinc oxide or titanium dioxide sit on the skin surface and work better for skin prone to perioral dermatitis.
Why Perioral Dermatitis Starts Suddenly
The rash often appears without an obvious cause. Most of the time, something changed recently, even if the connection isn’t obvious yet.
A new moisturizer, a different toothpaste, starting an inhaled steroid, or prolonged face mask use can all push a borderline barrier into a full flare. Face masks create heat and humidity that alter bacterial balance on your skin, and this became evident during the pandemic when perioral dermatitis cases increased significantly. Sun exposure and wind add further stress to an already compromised barrier.
Hormonal shifts are another common culprit. Some women notice perioral dermatitis worsens in the days before their period, and birth control pills trigger flares in certain individuals. Estrogen and progesterone fluctuations affect both barrier function and inflammation pathways, which is why the rash can appear suddenly during hormonal transitions even when nothing else has changed.
Diet and Gut Health
Research on the gut-skin axis suggests dysbiosis may contribute to inflammatory skin conditions including perioral dermatitis, though clinical trials specific to this condition don’t exist yet. Many people notice flares after certain foods and improvement when they eliminate them.
Common dietary triggers include dairy, gluten, refined sugar, and alcohol. Gastrointestinal symptoms alongside perioral dermatitis may indicate gut microbiome imbalance worth discussing with your doctor.
If you notice a pattern between specific foods and your flares, an elimination approach is worth testing. Remove suspected triggers for four to six weeks alongside the trigger elimination steps in the next section, then reintroduce one food at a time to identify your personal triggers.
How to Get Rid of Perioral Dermatitis at Home
Eliminating triggers comes before adding any treatments. For mild cases, this alone clears the rash. For severe cases, it makes prescription medications work faster and more reliably.
Stop all topical steroids – Follow the gradual tapering approach in the previous section. Stopping abruptly triggers rebound flares that set you back significantly.
Switch your toothpaste – Replace fluoride toothpaste with a fluoride-free alternative. Tom’s of Maine and Burt’s Bees both make widely available options. Eliminate breath mints, chewing gum, and mint lip balm too, since these maintain constant irritation around your mouth.

